P-Valve
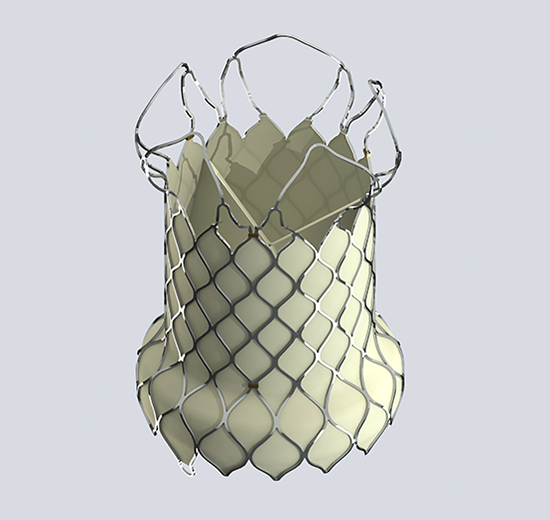
The Venus P-Valve System is the first self-expanding nitinol stent for pulmonary valve in Europe known to Venus Medtech.
Explaination
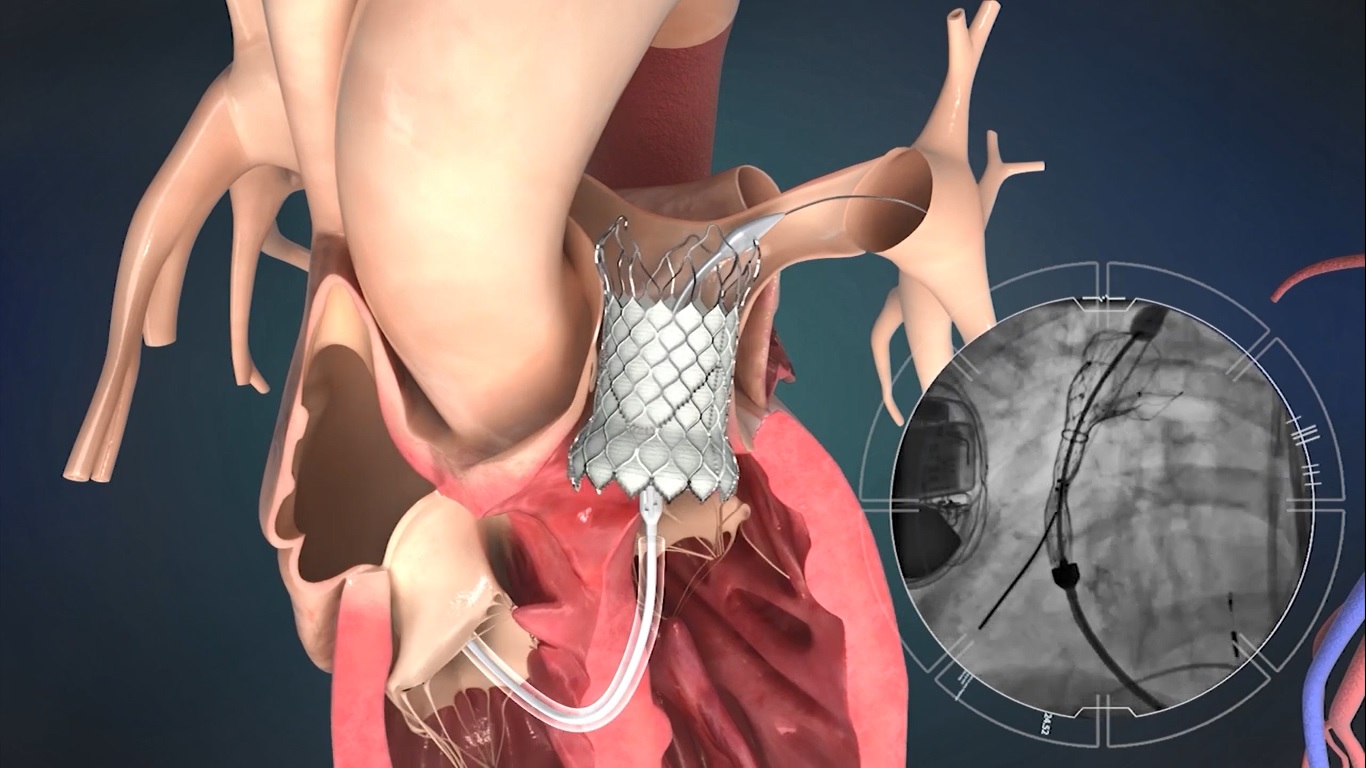
The VenusP-Valve System was designed at 28-36 mm for valve diameter specifically for large RVOTs. The intended purpose of VenusP-Valve is to replace the pulmonary heart valve with an artificial valve using a minimally invasive percutaneous approach, to treat right ventricular outflow tract (RVOT) dysfunction and specifically for the dilated outflow tracts to restore pulmonary valve function.
Pulmonic Valve disease
Congenital defects involving the RVOT require iterative surgical interventions and/or corrections throughout a patient’s growing years and young adulthood. Some of the defects include pulmonary atresia and pulmonary stenosis. Other defects that are more complex and require complex surgeries. Tetralogy of Fallot with pulmonary atresia, truncus arteriosus, double outlet right ventricle or a single pumping chamber combined with multiple complex anomalies. Some congenital defects of the aortic valve are corrected by replacing the failing aortic valve with the patient’s own (native) pulmonary valve. When this is done, a conduit is placed in the RVOT to support pulmonary flow. This procedure is known as the Ross procedure.
There are many types of conduits used for surgery. The current valves available in the market are not suitable to treat many of the needy patients. Re-intervention options for chronic pulmonary regurgitation in the setting of previous RVOT patching are currently limited to surgical valve replacement as current balloon expandable transcatheter valves are not large enough for the dilated native RVOT. Significant challenges have been identified with providing a single self- expanding system that will function over the wide variety of post-operative anatomical variants that exist within this setting.